Central Valley Periodontics & Implants -
Referral Implant
Autosave
Save For Later
Download Options
Download As PDF
Print Form
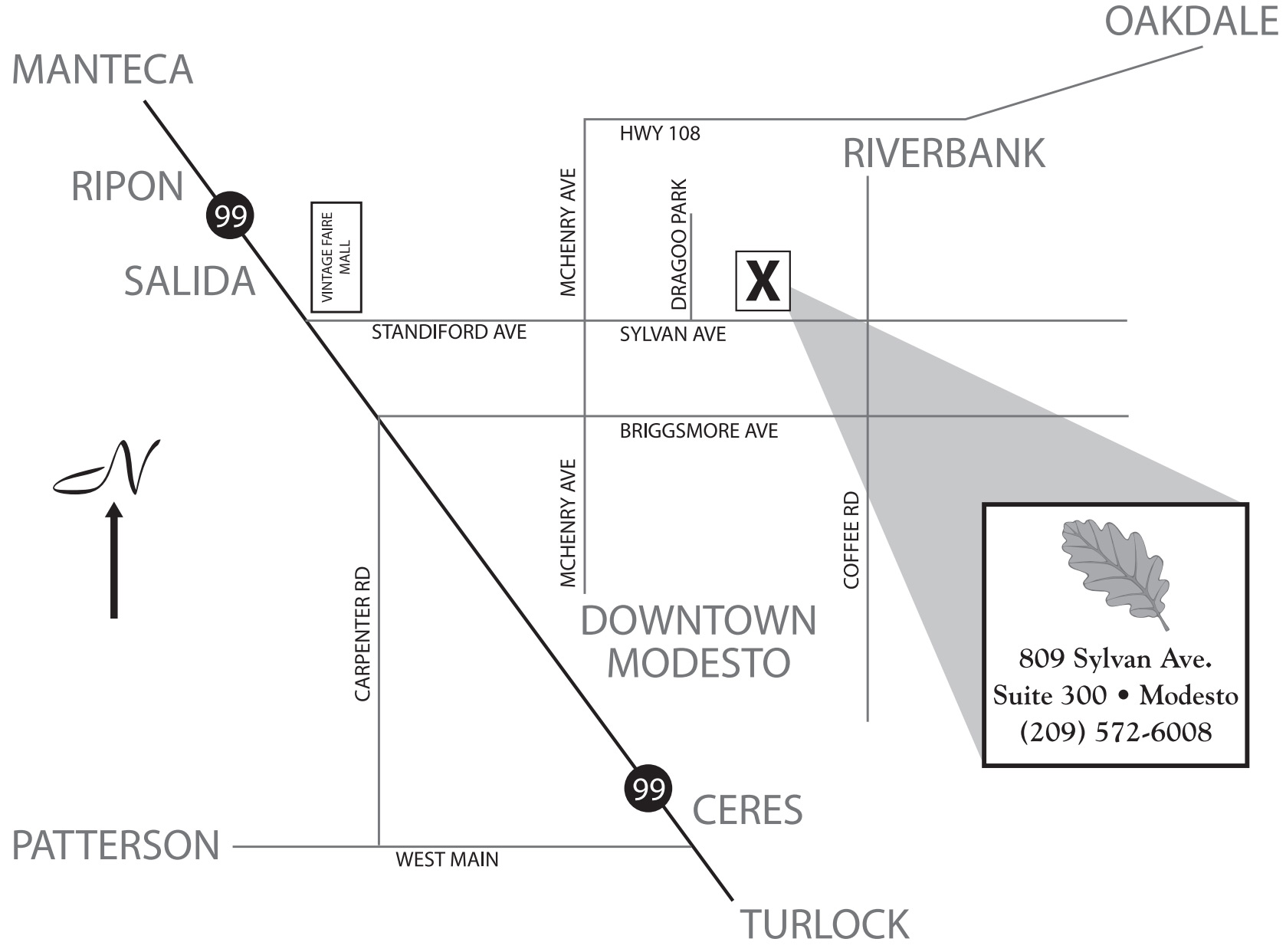
809 Sylvan Ave., Suite 300, Modesto, CA 95350
209-572-6008 | Fax: 209-572-6009
https://www.centralvalleyperio.com
IMPLANT REFERRAL
PATIENT NAME
PATIENT PHONE NUMBER
REFRERRED BY (DOCTOR)
REFERRAL DATE
APPOINTMENT DATE
Evaluation
SELECT IMPLANT SITES:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
32
31
30
29
28
27
26
25
24
23
22
21
20
19
18
17
SELECT TEETH TO BE EXTRACTED:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
32
31
30
29
28
27
26
25
24
23
22
21
20
19
18
17
IMPLANT SYSTEM:
Periodontal or mucogingival considerations?
YES
NO
Would you like a telephone call during the patient's appointment?
YES
NO
TENTATIVE RESTORATIVE PLANS:
Single Unit Crown
Fixed Bridge
Over-denture
Radiographs
Enclosed please find all radiographs available from my office.
I have no radiographs. Please take what you will need.
Our office will email radiographs to xray@centralvalleyperio.com
Comments
Patient Validation
(Your name needed to submit online form)
Prev
Next
Submit Form
Signature
Processing